
Phantom-based training of ultrasound-guided breast biopsy in medical education: a randomized controlled trial comparing handheld and high-end ultrasound | BMC Medical Education

Study design and participants
This single-center prospective randomized study was conducted at the Department of Radiology at the University Medical Center Regensburg between April 2024 and August 2024 after institutional review board approval. As this educational study did not involve clinical interventions it was not prospectively registered (Clinical trial number: not applicable). Medical Center teaching staff of the School of Medicine invited 120 medical students who had passed the first state examination and had attended a standardized training in diagnostic US. Obligatory for inclusion was the completion of two consecutive ultrasound courses in a near-peer-teaching setting, addressing basical as well as advanced knowledge of performing standardized ultrasound examinations on various body parts, though not covering interventional US-techniques so far [14, 15]. 32 medical students participated as volunteers in the study and written informed consent was obtained before study inclusion. Participants were randomly assigned to one of the two groups, the HUD-group or HEUS-group, using an envelope randomization strategy (Fig. 1).
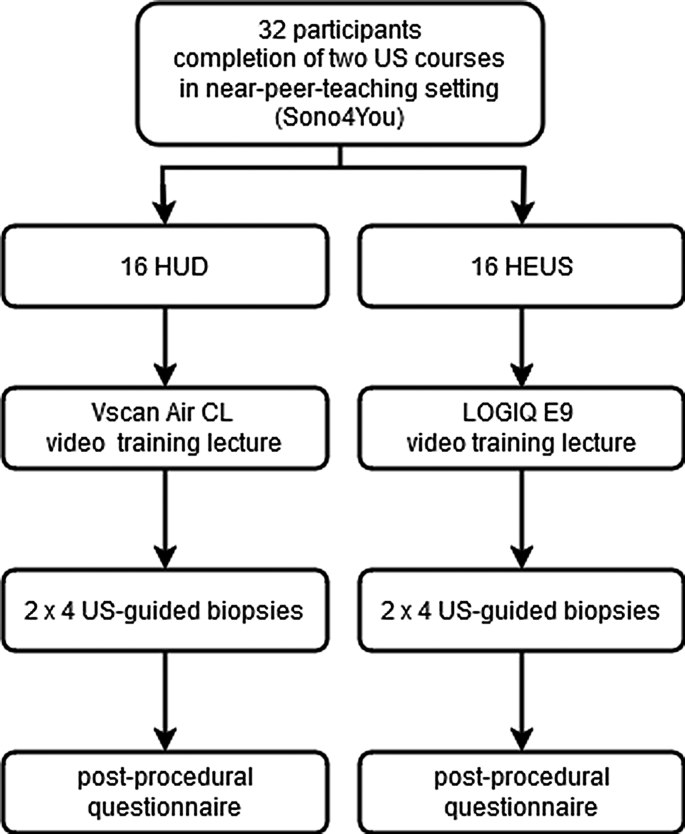
Diagrammatic representation of the study design
The time slots, for which the participants were scheduled, were assigned to the HUD-group or HEUS-group by drawing envelope-concealed numbered assignment slips from an opaque pouch.
At the scheduled time slot the participants viewed one of two prerecorded training videos (approx. 9 min) providing a general overview of how US-guided interventions are performed and showing the specific task the participants were to perform (video #1 for using LOGIQ E9, and video #2 for using Vscan Air CL; both US-devices by General Electric Healthcare, Chicago, USA). The structure of the breast phantom and the target lesions were presented in the video. For standardization purposes participants received training solely through video presentation. Each participant watched the assigned video alone in a room, pausing or repeating it in whole or in part was not allowed. They could familiarize themselves with the assigned US-devices, using the linear probe of LOGIQ E9 with a frequency range of 9-14 MHz or Vscan Air with a frequency range of 3–12 MHz, the transparent and opaque breast phantoms (Kyoto Kagaku, Kyoto, Japan; Fig. 2c) and the biopsy needle (Achieve 14G, 11.0 cm long, Merit Medical, Limburg, Germany) during the video lecture and up to 5 min afterwards. The HUD was connected via WLAN to an ipad (Apple Inc., Cupertino, USA) solely serving for this purpose (Fig. 2a).

Successful biopsy. Post-fire image using handheld ultrasound guidance in a. Needle depicted in hyperechogenic lesion (arrow). Core sample with blue colored material indicating successful biopsy in b. Opaque (left and transparent (right) breast phantom in c
Afterwards the participant scanned the breast phantom in B-Mode for identification of 4 target lesions: One 10 mm hypoechogenic and one 10 mm hyperechogenic lesion in the nipple-near part of the phantom, one 6 mm hyperechogenic lesion in the middle and one 10 mm hyperechogenic lesion in the deeper part of the phantom (Fig. 3). All participants had to biopsy the same 4 lesions in the same order starting with the 2 more superficial lying lesions and ending with the lesion in the deeper part of the phantom.
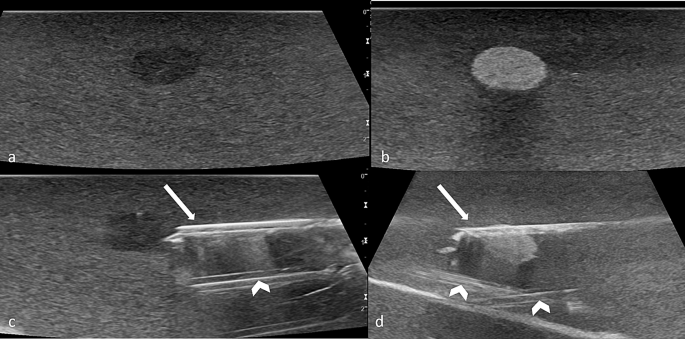
Target lesions. Hypoechogenic lesions in a and c, hyperechogenic lesions in b and d. Biopsy needle (arrows) pre-fire in c, post-fire in d. Hyperechogenic channels from previous biopsies (arrowheads)
Once a target lesion was identified and adjusted, the preloaded biopsy needle was freehand-inserted into the phantom by the participant under US-guidance either using the HUD or the HEUS. At this timepoint (contact of the needle tip with the surface of the phantom) a timer was started by a supervisor, who was present in the same room without interacting with the participant. Time measurement was finished as soon as a core biopsy was obtained by firing the biopsy needle (Fig. 2a). A biopsy was deemed successful if any colored lesion material was present in the core sample (Fig. 2b). Four phantoms were used for the study (2 in each group) and the phantoms were exchanged for a new one in the middle of the study after the eighth participant in both groups. It had been outlined in the video training how to differentiate between tracks by prior biopsies and the inserted biopsy needle.
The procedure was repeated two times for each of the four lesions (in total 8 times per participant). Following the biopsy procedures, all participants were asked to complete a post-procedural questionnaire (Supplemental Fig. 1). For evaluating and assessing the participants` subjective impressions in the trial they had to record their personal experience in three categories. The Raw NASA Workload Task Load Index (TLX), a subjective, multidimensional assessment tool was used to rate the participants` perceived workload [16, 17]. The questionnaire`s design was chosen to be simple to facilitate the students´ assessment and minimize interobserver variability between the evaluators. Moreover, the standardized protocol including video-based training with as little interaction between observers and participants as possible and the choice of objective and simple parameters as primary outcomes were important factors addressing interobserver variability. For these reasons, the interobserver variability was not quantified.
Primary outcomes
Primary outcomes of the study were the rate of positive biopsies per student and the skin-to-fire-time for each lesion.
Secondary outcomes
The subjective assessment of the operability and safety of US imaging and biopsy guidance devices and individually perceived workload were defined as secondary outcomes. Directly after the biopsies were taken, the participants had to record their personal impressions in three categories with a 6-point Likert scale (0–5; 0 = absolutely comfortable/safe and not difficult at all, 5 = not at all comfortable resp. safe and very difficult): (1) Comfort (“I felt the imaging system used was comfortable for me”), (2) Safety (“I felt safe performing the biopsy while using this ultrasound imaging system“, regarding orientation, needle firing and tissue asservation), (3) Difficulty (“Overall difficulty of the task“). The assessment of the mental workload was performed with the Raw NASA Task Load Index (NASA TLX). Mental, physical and temporal demand, performance, effort and frustration of the participants were assessed on a 20-point Likert scale (1–20; 1 = very low, 20 = very high).
Statistical analysis
Frequencies are presented as absolute numbers and percentages. Continuous data are presented as median values and interquartile ranges (IQRs). Differences between the groups were analyzed using the Pearson chi-square test of independence for dichotomous parameters and the Wilcoxon-Mann-Whitney U test for continuous data. A p-value < 0.05 was considered statistically significant. All analyses were performed using SPSS version 29.0.1.0 (IBM, NY, USA).
link




